
What Every Pharmacist Should Know about Erectile Dysfunction
(Image)
Steph’s Note: Sorry for the brief, unplanned hiatus, but we’re back this week! And given this week marks the rollover to the new year and people are going to be par-taying it up on NYE, let’s have some real talk. About sex.
Nope, this isn’t going to be the birth control chat. (We’ve already done that in this post.) This is going to be a matter-of-fact discussion about male sexual dysfunction. So many of us probably dispense and check those little blue pills every day (or add them to medication lists), but do you really know how they work? Or how extensive the assessment for patients requiring these therapies should be? We frequently skim over this topic - often because patients (understandably) are uncomfortable providing details, but today’s the day to (tactfully) dig deeper. So let’s get the party started!
Anatomy and Physiology of Male Sexual Function
You probably learned most of this in your undergraduate anat/phys course, but if you’re like most of us, you probably also dumped it right after your final exam. And then you learned it again in pharmacy school…only to dump it once more. Because how often do you really need to think about male sex hormones?
Well, you do today. So here you have a quick refresher.
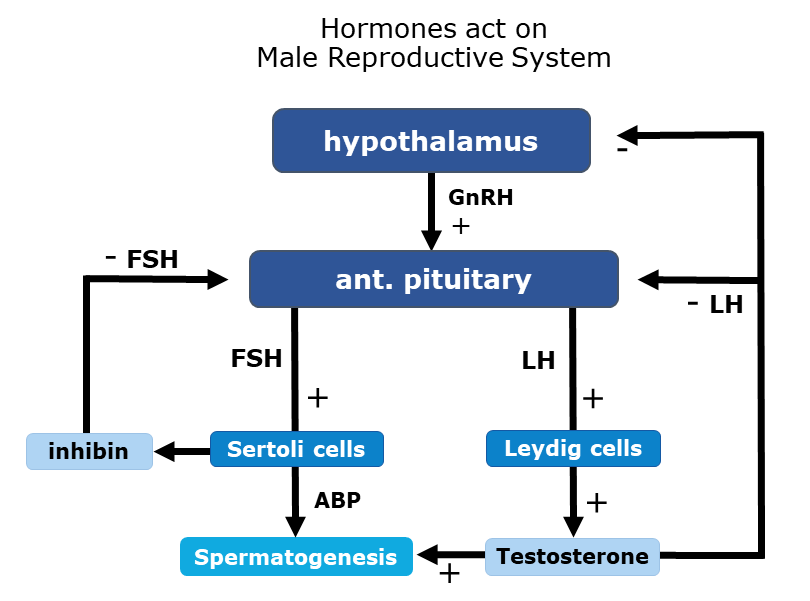
There are 3 hormones involved in male sexual function:
(Image)
Follicle-stimulating hormone (FSH): stimulates testosterone hormone uptake in the Sertoli cells of the testes and therefore spermatogenesis; made in the pituitary gland
Luteinizing hormone (LH): stimulates testosterone production and spermatogenesis; also made in the pituitary gland
Testosterone: helps with development of male sex traits (e.g., muscle mass, bone mass, sex drive. etc) and spermatogenesis; largely made by the Leydig cells in the testes but also in the adrenal glands
Check out the figure above for a summary of how these hormones work in concert.
In terms of anatomy, there are both internal and external organs. Check out the brief descriptions below to refresh how these parts work together to enable males to have sex and urinate.
External Male Reproductive Anatomy

(Image)
Penis: the male organ for sex. Has specialized, spongy cavities inside called the corpora cavernosa, which fill with blood during arousal to produce an erection. Another side benefit of this fullness during intercourse is the blockage of urine flow through the urethra (the ultimate traffic control, right?). There’s also the corpus spongiosum, another spongy cavity that surrounds the urethra.
Scrotum: the ball-like sac behind the penis that holds the testicles (testes), nerves, and blood vessels. It is responsible for keeping the testes at the optimal temperature for sperm development. It’s a rather finicky process and requires temps to remain between 97-99*F, so specialized muscles will actually contract or relax to move the scrotum closer or further away from the body as needed. Evolution is pretty cool, isn't it.
Testicles (testes): these make testosterone and produce sperm in the seminiferous tubules.
Epididymus: transports and stores the sperm made in the testes. It also helps with maturation of the sperm since sperm straight from the testes are not yet capable of fertilization.
Internal Male Reproductive Anatomy
Vas deferens: the tube that transports mature sperm from the epididymus to the urethra for ejaculation.
Seminal vesicles: produce ~80% of ejaculatory fluid, including fructose, which provides an energy source for swimming sperm.
Ejaculatory ducts: the vas deferens terminates in these, which move sperm through the prostate and into the urethra.
Prostate: when it comes to male sexual function, this organ produces a fluid that is added to the sperm when it passes through. Sperm + seminal vesicle fluid + prostate fluid = semen.
Urethra: the tube that carries both urine and semen outside the body. Of note, this runs through the prostate gland.
Alright, now that we have the hormones and anatomy down pat again, let’s talk about how it all works.
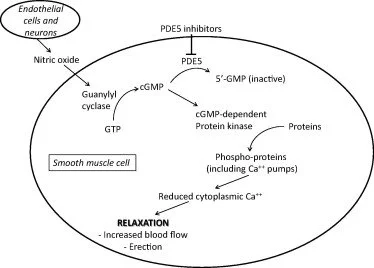
Note the involvement of nitric oxide in activating guanylyl cyclase, which increases production of cyclic GMP. Through a series of additional steps, cGMP eventually leads to smooth muscle relaxation. Phosphodiesterase 5 (PDE5) is the check and balance to this process. It is the enzyme that degrades cGMP into inactive 5’-GMP. (Image)
Generally, the male sexual cycle is defined as 4 phases: desire, arousal, orgasm, and resolution. Because this post is about ED, we’re going to focus on step 2, arousal.
During arousal, in response to stimuli (aka whatever floats your boat), there’s both a parasympathetic nervous system and molecular response. The parasympathetic response comes from the S2-S4 of the sacral spine.
The molecular response is mediated by nitric oxide (NO), which leads to smooth muscle relaxation and vasodilation. This is what allows for increased blood flow to the corpora cavernosum and corpus spongiosum, leading to an erection.
Now that we know how things normally operate to create an erection, what happens when it just doesn’t work…
What is Erectile Dysfunction (ED)?
According to the 2018 American Urological Association guidelines for treatment of ED, erectile dysfunction (ED) can be defined as “an impairment in the arousal phase of sexual response and is defined as the consistent or recurrent inability to attain and/or maintain penile erection sufficient for sexual satisfaction, including satisfactory sexual performance.”
An estimated 30 million men in the US and up to 150 million men worldwide are thought to be impacted by ED. Based on the 2022 census, there were over 165 million men in the US, so that’s almost 20% - a FIFTH - of the American male population that’s affected by ED.
Why aren’t we talking about this more??
Not to mention, ED is extremely tightly intertwined with cardiovascular disease. They have many of the same risk factors, including smoking, diabetes, hypertension, obesity, hyperlipidemia, and sedentary lifestyles. Plus, ED may actually be a prognostic factor for a CVD event! Evidence shows that ED may precede a CVD event by up to 5 years, and young men with ED have up to a 50 fold higher risk of CVD in the future.
The presence of ED should prompt health care providers to take a closer look at potentially undiagnosed or undertreated chronic health conditions. More than likely, it’s not just ED.
Talk about a canary in the coal mine, wouldn’t you say? THIS is why we’re talking about this today.

(Image)
ANNNND… let’s just have a moment to consider the other systems impacted by ED. Number one, mental health. Number two, relationship health. Let’s be real - sex is a normal part of the human experience, and when it isn’t working (not that uncommon, btw, as we’ve discussed), it can mess with your head…and your partner’s head too.
Once a patient has been thoroughly assessed and diagnosed with ED, it’s time to determine an appropriate initial therapy. Options range from pharmacotherapy to mechanical, but we’ll be focusing on the medications for this post.
Treatments for Male Erectile Dysfunction
Oral Phosphodiesterase-5 Inhibitors for ED
Often the first-line treatment options for ED are the oral phosphodiesterase-5 (PDE5) inhibitors. In the US, we have sildenafil, vardenafil, tadalafil, and avanafil. These all work similarly in that they block the PDE5 enzyme from breaking down cGMP, which allows for a continued cascade to eventual smooth muscle relaxation and vasodilation of the arterioles supplying the penis. One key note here is that patients have to have intact penile vasculature for these medications to work.
All of the PDE5 inhibitors in the US have similar efficacy except potentially avanafil, for which published data is limited. So how to choose?
Well, pharmacokinetics plays a large role here. Check out the chart below to see which medications kick in faster, which don’t last as long (could be beneficial in people with comorbities), and which may offer more flexibility for the user.

A few notes here… This is absolutely a case of use the lowest effective dose possible. So even though I’ve provided usual starting doses, some patients may not need (or may not tolerate) that much, and decreases are possible. Also, when working on finding a patient’s effective dose, the dose-response relationship is small and NOT linear. Meaning that changes in dose usually produce small results, and if you double a patient’s dose, they do not get double the effect.
Patients should be counseled that it’s common to require multiple dosing changes to find the right one. So they shouldn’t feel discouraged if it doesn’t do the trick right away! It’s also not uncommon for patients with more severe ED (e.g., post-prostatectomy or diabetic) to start at higher doses (assuming they are not high risk for adverse effects).
Another thing that is often misunderstood about these medications is that they do not make a man have an unprovoked erection. They allow for an erection to occur in the presence of a man’s desire (again, whatever floats his boat). So it’s not like take a dose, and whoop, there it is in an hour or whatever regardless of the situation or environment. Rather, it’s take a dose, and the ability to have sex is available in that timeframe, if and when desired.
Don’t let the movies fool you. They already do that enough with awful, misleading depictions of CPR.
Next, you may have noticed in the chart above that tadalafil is the only PDE5 inhibitor to have 2 dosing options. One of these is on-demand PRN dosing and the other is daily dosing regardless of timing of sex. It’s the only PDE5 inhibitor approved for daily dosing, and efficacy appears to be similar between the 2 regimens.
Choosing between these is purely patient-specific. Do they want to take a pill every day and not have to think about timing for sex? Or is taking it every day too much to remember, and they just want to take it when they need it? Or did they try the on-demand option and experience adverse effects from the higher dose, such that they want to try the lower dose daily option? Or do they have comorbidities that warrant an off-drug period to decrease risk of adverse effects?
On that note…let’s talk about contraindications and warnings for PDE5 inhibitors.
So we’ve talked about how these medications cause increased blood flow to the penile vasculature. Useful for treating ED, obviously. Not so useful for patients who suffer from low blood pressure or who take medications that could increase the risk of hypotension.
The big class of medications that we most often hear about interacting with PDE5 inhibitors to cause dangerous drops in blood pressure are the nitrates. Think isosorbide for hypertension or heart failure patients. Think PRN nitroglycerin for angina. Men who take nitrates regularly really shouldn’t use a PDE5 inhibitor, and those who use sublingual PRN nitroglycerin should be carefully considered depending on how often they reach for this medication. They should also be counseled not to use their pocket nitro within 24 hours of a PDE5 inhibitor (or even longer in the case of tadalafil’s long half-life).
When the team asks you to evaluate a patient’s extensive medication list for possible drug interactions #pharmacynerd (Image)
Alpha blockers are another class of medications that can have significant effects on blood pressure in combination with the PDE5 inhibitors. Many of the dosing recommendations for these drugs are affected by concomitant use of an alpha blocker. And guess what…considering a lot of our ED patients are older males who also have prostate issues, this alpha blocker issue is not a rare unicorn.
Speaking of drug interactions, the PDE5 inhibitors are major substrates of CYP3A4 for their metabolism. So you can probably already guess the plethora of drug interactions here: antifungals, antiretrovirals, antidepressants, antihypertensives, etc. It’s a doctor’s nightmare (and a pharmacist’s dream)!!
Dosage adjustments, especially initially, should also be implemented for patients with severe renal and hepatic impairment. Again, we’re often treating the older male population, for whom these are not uncommon comorbidities!
Outside of the blood pressure issue, PDE5 inhibitors are generally well tolerated with only mild to moderate adverse effects. These can include upset stomach, flushing, headache, dizziness, back pain, nasal congestion, and visual disturbances.
Alright, now that we’ve covered the oral, first-line options for treatment of ED, it’s time to dig even deeper into the therapy lines.
Intraurethral Alprostadil for ED
Even though we all think of the PDE5 inhibitors first for ED, there are patients for whom these aren’t appropriate due to contraindicated medications or medical conditions. There are also patients who aren’t able to tolerate those medications or people who wish to not have to take a pill. And then there’s the estimated 40% for whom they just plain don’t work. So what then? Are they SOL?
Nope, fear not! We have more treatment options.
The next treatment option available is intraurethral alprostadil (Muse Pellet). Let’s take this in 2 pieces. First, intraurethral means that the pellet medication is delivered directly into the urethra by a catheter device. Second, alprostadil is prostaglandin E1. When delivered via the urethra, alprostadil causes smooth muscle relaxation and dilation of the arterioles in the corpora cavernosum. This allows for increased blood flow to the penis and subsequent erection.
The intraurethral initial dose is 250 mcg delivered as needed to achieve effect, and doses may be titrated up from there. It comes in 3 strengths, 250 mcg, 500 mcg, and 1000 mcg, BUT only 2 systems should be used per 24 hours. Onset of action is between 5-20 minutes, and duration of action is less than an hour.
Not a whooooole lot of flexibility for this one, is there? Have to have your timing more honed in for this one.
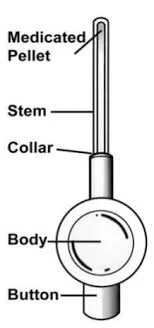
The Muse intraurethral applicator. (Image)
As you might guess, patients have to be properly instructed on how to use the transurethral device. A few important counseling points include the following:
Patients should be instructed to urinate prior to insertion as the residual urine in the urethra helps to dissolve and disperse the alprostadil pellet.
Intraurethral alprostadil is contraindicated in anyone with abnormal penile anatomy (you can imagine that insertion of the suppository would NOT go well in these cases…).
This medication is contraindicated in anyone at increased risk of venous thrombosis and/or priapism, including those with hyperviscosity conditions (e.g., sickle cell, thrombocythemia, polycythemia, or multiple myeloma).
Alprostadil is embryotoxic, so intraurethral alprostadil should not be used for sex with pregnant women UNLESS a condom barrier is also used.
Foil pouches containing the medication and device should be stored in the refrigerator, OR they may be used within 14 days of warming to room temperature.
Adverse effects are mostly hypotension, dizziness, and possible syncope, which is also why initial dose titration should occur in a health care provider’s office. Priapism (a rigid erection lasting at least 4 hours), while rare at recommended doses, is also possible. Some patients also reported urethral and penile discomfort upon insertion, and some also had some spotting/bleeding, which was a deterrent to continuing therapy.
Interestingly, intraurethral alprostadil is largely metabolized by local enzymes, and so it is not significantly detected in systemic circulation. This makes it less of a candidate for major drug interactions, although antihypertensives may independently add to the risk of hypotension.
There you have it. Treatment option class #2 for ED. Are we out of options now? Nope!
Intracavernosal Injections (ICI) for Treatment of ED
Another line of therapy (I hesitate to deem it third line since that seems to imply lesser efficacy, which isn’t necessarily true…) are intracavernosal injections (ICI). These are medications that (as you likely guessed) are injected directly into the intracavernosal cavities of the penis to produce an erection. Although alprostadil is the only FDA approved option for ICI in the US, other injected medications include papaverine, phentolamine, and atropine. And these are often injected together in varying combinations…
Since we’ve already talked about how alprostadil works, let’s take a quick look at the other medications and how they might contribute to a successful erection.
Papaverine causes smooth muscle relaxation, possibly through increasing levels of cyclic AMP. It’s not really used much anymore for its original labeled uses of vascular spasm and vasospasm, but you may see a vial of this in an OR pharmacy for local administration during coronary artery bypass graft (CABG) surgery.
Phentolamine is an alpha-adrenergic receptor blocker (alpha blocker) that produces vasodilation by inhibiting the action of the catecholamines (epinephrine and norepinephrine). You’re most likely to see this on an extravasation management flowchart for local vasopressor extravasation.
Atropine is an antimuscarinic anticholinergic medication that produces smooth muscle relaxation in the cavernosal tissue at higher concentrations. You’re most likely to see this in your hospital’s code box for symptomatic and/or hemodynamically unstable bradycardia.
We’re not going to go too far into the weeds on this option as it’s largely completed under the direction and tutelage of a urologist, but here are a few important notes.
First, pain is one of the most reported side effects. Not exactly a big surprise. It certainly doesn’t sound pleasant, does it… Second, less expected but also logical is the potential for penile fibrosis and/or deformities with continued injections. It’s not clear at this point whether one or more of the injected medications carries a higher risk for this possibility, so documentation of baseline conformation is recommended for monitoring purposes.
See, now you know why we had to review anatomy at the beginning of this post! Helps to understand how and where these therapies are working. Other therapies include non-pharmacologic options like a vacuum erection device (VED) or a penil prosthesis implant. It should also be noted that testosterone replacement may play a part in treatment of ED for those who have low levels, but that would be a whole other discussion. And this is tl;dr after all. I’m already flirting with that designation as it is.
So let’s wrap up.
The tl;dr of Erectile Dysfunction for Pharmacists
Knowledge of the male reproductive anatomy and hormonal processes is useful for pharmacists who encounter men requiring treatment for ED. Patients diagnosed with ED should be assessed for mental health, as well as possible contributory and consequent comorbidities, including CVD.
Treatments for ED include the PDE5 inhibitors, intraurethral alprostadil, and intracavernosal injections. By and large, PDE5 inhibitors are the most commonly utilized therapies, and pharmacists should be familiar with their basic pharmacokinetics, counseling points, and drug interactions in order to ensure therapy is safely optimized. Dosage adjustment will be necessary without a doubt, and patients (and partners!) should be instructed not to be discouraged by the process.
Should PDE5 inhibitors fail or be contraindicated, intraurethral alprostadil or intracavernosal injections may be attempted under the guidance of a urologist.
So there you have it - erectile dysfunction in a nutshell. Happy New Year to y’all, and we’ll see you for more fun learning next year!

(Image)